EMAT Cases
Case Description
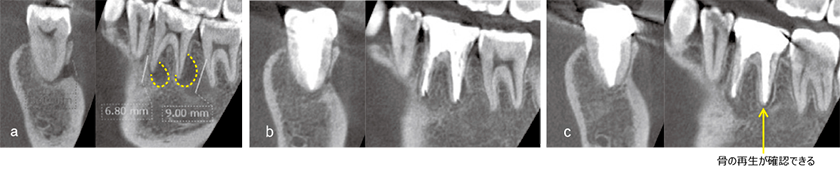
A 6 root tip lesion had spread buccally, perforated the buccal bone, and formed a thin canal with an opening diameter of approximately 3.7 x 5.8 mm. Bleeding was observed from the distal root canal foramen, and the probing depth was within 3 mm. After root canal formation, EMAT was performed and the canal was filled immediately. Although there was a slight enlargement of the periodontal lumen on the distal side of the centorhombic root, the bone beam structure was homogenized, and a continuous alveolar hard line was observed, showing an almost normal image.
It is known that the thin hole usually heals after appropriate root canal treatment and resolution of periapical inflammation. However, when the bone wall defect is large, bone formation is insufficient and connective tissue invades the defect, resulting in some cases where bone defects remain on radiographs despite the absence of inflammation.
In this case, a large bone wall loss was observed on the buccal side, but bone formation was observed one month later, suggesting that EMAT may have exerted its healing-promoting effect.
Case Description
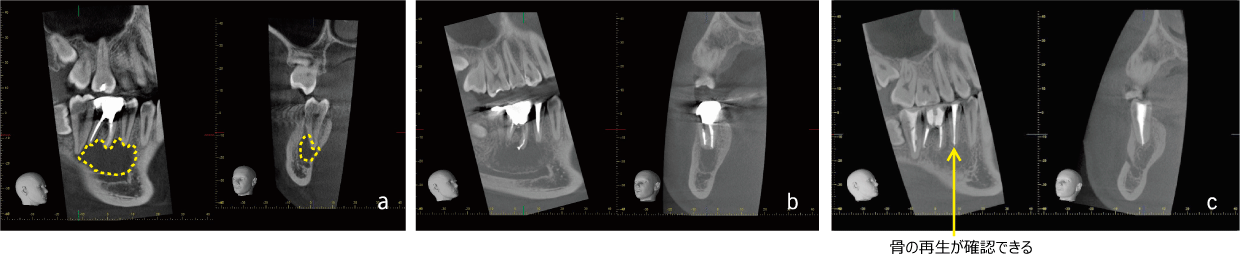
An X-ray transmission image with a width diameter of approximately 26.5 mm was observed in the white tooth area on the right side of the mandible, and root canal treatment had been performed on 6┐. The electro pulp examination revealed that 7┐ and 5┐ did not show any signs of living reaction, so root canal treatment was performed on the three teeth according to the usual method. After removing the contaminated contents and dentin from the root canal, passive ultrasonic irrigation was performed using 2% sodium hypochlorite. The patient underwent passive ultrasonic irrigation using 2% sodium hypochlorite, and calcium hydroxide was applied three times, but there was no significant change in the findings in the root canal. Therefore, the 6┐ proximal root tip equivalent was dissected with a 5×5 mm full-layer valve, the buccal bone was perforated by approximately 3-4 mm, and EMAT was performed through the 65┐ root canal after a possible curettage of the cyst wall with the aim of promoting bone formation. After 3 months, osteogenesis was already seen in the bone wall of the lesion, and after 2 years and 1 month, the bone trabecular structure was almost equal to that of the surrounding bone.
Although it is often reported that the size of the lesion affects the success rate of treatment, we believe that the fact that the bone defect improved in 3 months may be due to the healing-promoting effect of EMAT, even though curettage of the cyst wall was also used in this case.